Out-of-pocket expenditure (OOPE) refers to direct payments individuals make for healthcare services, medications, and treatments not covered by insurance or government programs. High OOPE can significantly impact individuals, especially in healthcare, where unexpected costs can be financially burdensome.
India’s progress in reducing out-of-pocket expenditure
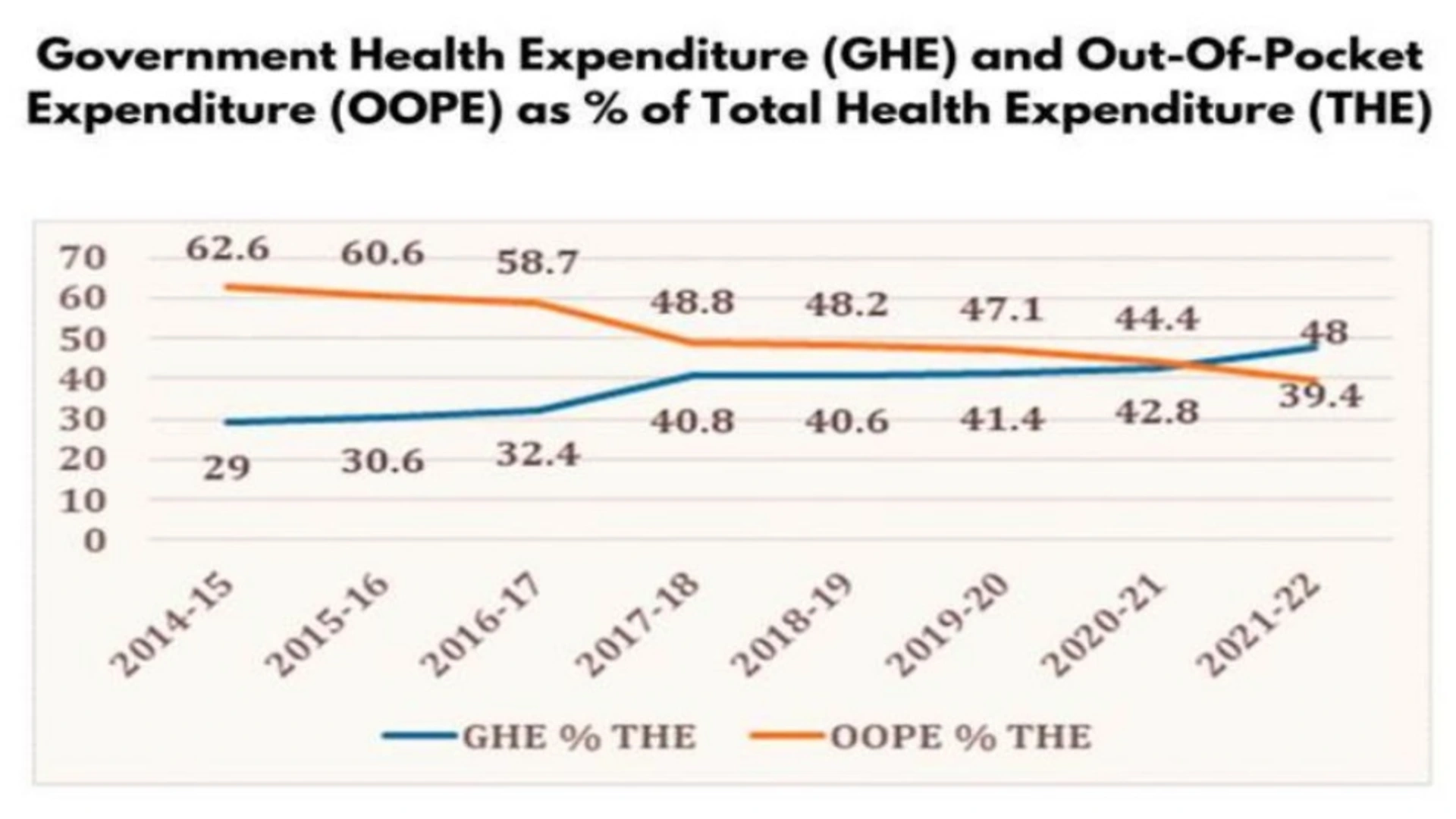
India has made strides in reducing OOPE, though costs remain relatively high compared to global standards. National Health Accounts (NHA) data for 2021-22 indicate a downward OOPE trend, attributed to increased government health expenditure (GHE) and initiatives like Ayushman Bharat. Despite this progress, OOPE still constitutes a substantial portion of healthcare spending, with many households bearing significant medical costs.
Historically, India has ranked among countries with the highest OOPE as a percentage of total health expenditure. In 2013-14, OOPE accounted for 64.2% of total health expenditure, declining to 39.4% in 2021-22.
Government health expenditure and its impact
The rise in GHE has played a central role in reducing OOPE. From 2014-15 to 2021-22, GHE as a percentage of GDP rose from 1.13% to 1.84%, and its share in total government spending grew from 3.94% to 6.12%. During this period, per capita health spending tripled from Rs 1,108 to Rs 3,169, enabling the government to strengthen healthcare infrastructure, making services more affordable and accessible, thus alleviating OOPE burdens.
Social security expenditure on health
The government has expanded social security expenditure (SSE) on healthcare, including insurance schemes like Ayushman Bharat and various state-level initiatives. SSE’s share in total health expenditure rose from 5.7% in 2014-15 to 8.7% in 2021-22. These schemes target economically vulnerable populations, reducing reliance on personal finances for healthcare.
State-wise variations in OOPE
OOPE varies across Indian states due to disparities in healthcare access, infrastructure, and economic conditions. NHA estimates for 2018-19 show states like Bihar and Uttar Pradesh have the highest OOPE as a share of total health expenditure, at 76.2% and 71.3%, respectively, while states like Himachal Pradesh and Delhi report lower rates, around 52.3% and 53.5%. These figures suggest a higher financial burden in certain regions, highlighting the need for targeted interventions.
| State/Union Territory | OOPE as % of THE |
|---|---|
| Bihar | 76.2% |
| Uttar Pradesh | 71.3% |
| Rajasthan | 69.5% |
| Madhya Pradesh | 68.6% |
| Jharkhand | 67.3% |
| Odisha | 66.5% |
| Chhattisgarh | 65.2% |
| Assam | 64.8% |
| West Bengal | 63.7% |
| Gujarat | 62.5% |
| Maharashtra | 61.4% |
| Karnataka | 60.2% |
| Tamil Nadu | 59.1% |
| Telangana | 57.6% |
| Kerala | 56.8% |
| Punjab | 55.9% |
| Haryana | 54.7% |
| Delhi | 53.5% |
| Himachal Pradesh | 52.3% |
Source: National Health Accounts Estimates for India (2018-19), Ministry of Health and Family Welfare
Breakdown of health expenditure types in India
Understanding healthcare expense categories clarifies the budgetary impact on households. Key types include:
| Type of Health Expenditure | Description | Examples | Key Challenges |
|---|---|---|---|
| Out-of-Pocket Expenditures | Direct payments without insurance | Doctor visits, diagnostic tests | High costs in private facilities |
| Preventive Healthcare | Expenses to prevent illness | Vaccinations, screenings | Often overlooked, limited coverage |
| Hospitalization Costs | Planned/emergency admission expenses | Room charges, surgery fees | Can lead to debt |
| Chronic Disease Management | Managing long-term conditions | Diabetes, hypertension meds | Lifelong burden, often uninsured |
| Pharmaceuticals | Drug spending | Prescription drugs, supplements | High costs for chronic conditions |
| Health Insurance Premiums | Payments for coverage | Private plans, government schemes | Limited coverage for many |
| Alternative Medicine | Non-allopathic treatments | Ayurveda, yoga | Mixed insurance availability |
| Dental/Vision Care | Oral/eye health | Cleanings, braces, glasses | Not covered by insurance |
| Mental Health Services | Psychological care | Therapy, psychiatric consultations | Stigmatized, costly |
| Rehabilitation | Recovery after surgery or illness | Physical therapy, prosthetics | Long-term costs, often uninsured |
| Home Healthcare | At-home medical care | In-home nursing, oxygen therapy | Expensive, often uninsured |
| Travel for Treatment | Accessing distant/specialized care | Travel, lodging | Significant for rural patients |
Impact of reduced OOPE
Programs like Ayushman Bharat are essential in making healthcare more accessible, easing financial burdens on low-income families, and enabling equitable healthcare access. Reduced OOPE supports better health outcomes and disease prevention, as individuals are less likely to delay care due to costs. This investment in health drives long-term economic growth and emphasizes human capital development.
Global comparison of OOPE
According to WHO’s Global Health Expenditure Database, the top 10 countries with the highest OOPE as a percentage of current health expenditure include:
| Country | OOPE as % of Current Health Expenditure |
|---|---|
| Afghanistan | 78.8% |
| Nigeria | 77.2% |
| Myanmar | 74.9% |
| Sudan | 74.0% |
| Yemen | 72.8% |
| Azerbaijan | 72.0% |
| Bangladesh | 71.8% |
| Pakistan | 71.6% |
| Cambodia | 70.9% |
| Egypt | 70.5% |
Healthcare financing in India
Since independence in 1947, India has transitioned from a system dominated by OOPE to a more structured model, though challenges remain.
Post-independence focus on public health infrastructure
Early healthcare efforts focused on public health infrastructure and infectious disease control. Limited government spending and a lack of structured insurance kept OOPE high, especially as private healthcare expanded.
Initial national health programs
India launched several vertical programs targeting diseases like malaria, tuberculosis, and leprosy, providing free treatment but lacking comprehensive coverage for all conditions.
Introduction of insurance schemes
Government health insurance schemes, like Rashtriya Swasthya Bima Yojana (RSBY) in 2008, aimed at low-income populations but had limited impact due to coverage and implementation challenges.
Ayushman Bharat
Launched in 2018, Ayushman Bharat marked a significant shift by covering 40% of the population through PM-JAY and establishing 150,000 health and wellness centers. The scheme expanded insurance and emphasized preventive care, reducing OOPE by lowering dependency on secondary and tertiary care.
Rise in government health expenditure
Between 2014 and 2022, government health expenditure as a percentage of GDP increased steadily. By expanding public healthcare funding and implementing Ayushman Bharat, India has reduced household financial burdens and OOPE.
Global comparisons with developed nations
India’s healthcare financing compared to developed countries highlights different impacts on public health and financial security.
Universal healthcare in developed nations
In countries like the UK and Canada, universal healthcare funded through taxes minimizes OOPE, accounting for around 15-20% of total healthcare spending, in contrast to India’s 39.4%.
Mixed models in other nations
Countries like Germany and Japan have mixed models with public and private options, resulting in lower OOPE due to extensive insurance coverage and government subsidies.
Developing countries with high OOPE
Developing nations like Nigeria and Bangladesh face high OOPE percentages, underscoring the need for robust public healthcare funding to reduce OOPE and improve healthcare access.
Path forward for India
India’s progression from OOPE reliance to increased government spending demonstrates the impact of financial strategies on public healthcare access. Expanding insurance coverage and strengthening public healthcare are crucial steps toward universal healthcare.





