A 75-year-old morbidly obese female patient with BMI of 43 (Obese class III) with history of diabetes and complaints of nocturnal dyspnea and breathlessness since last six months was admitted to Lilavati hospital in Mumbai. She was getting breathless on minimal activity. Doing her daily chores like taking a shower, moving from one room to another and sleeping at night were becoming impossible day by day. Her legs had swollen upto her knees. She was diagnosed with severe mitral stenosis and mitral regurgitation. Patient was found to be high risk for surgery.
The 2D echocardiography confirmed severe mitral annular calcification, severe mitral valve stenosis with severe pulmonary hypertension. The patient was refused an open-heart surgery as she was at very high risk and in operable due to severe mitral annular calcification. Trans catheter Mitral Valve Replace ment (TMVR) is an option for patients with severe mitral valve stenosis and no surgical options. Mitral valve stenosis causes narrowing of the valve that restricts the blood flow into the main pumping cham ber of the heart. As a result, pressures build in the lungs and water start collecting in the lungs and legs. As a result patients develop breathlessness.





In some patients, while re placing the heart valve with a catheter, the heart’s anatomy gets in the way causing the heart leaflets to push back, thus blocking the blood flow and obstructing the left ventricular outflow tract (LVOT) which remains a common and often fatal complication in TMVR. Therefore, careful preprocedural computed tomography (CT) was done to define the risk of LVOT obstruction and plan a preventive strategy.
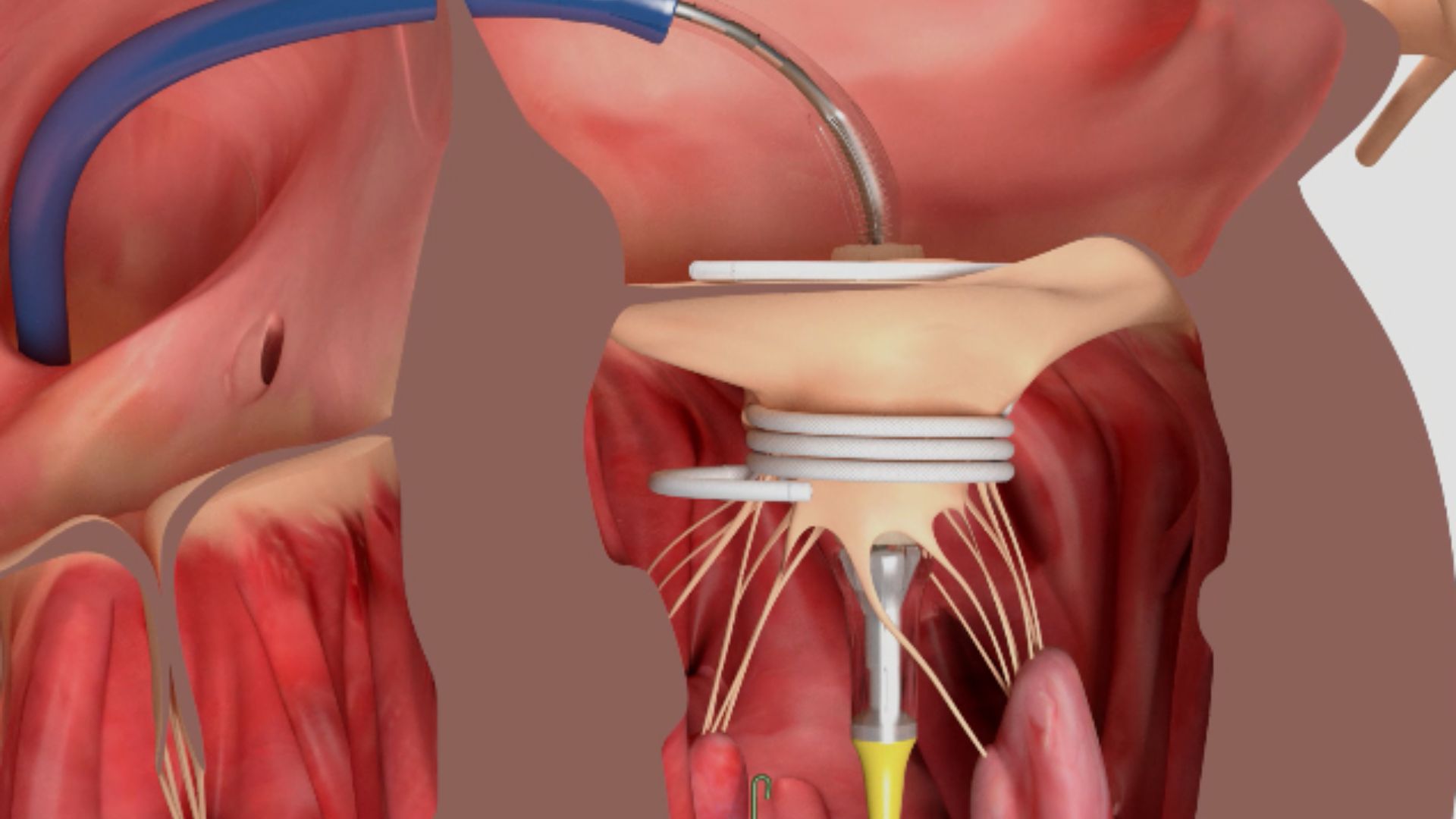
After thorough examination and analysis of the CT, ante grade intentional laceration of the anterior mitral leaflet (LAMPOON) was decided to be performed on the patient. LAMPOON is a transcatheter electrosurgical technique to split the anterior mitral valve leaflet immediately prior to TMVR procedure in patients at risk of LVOT obstruction. This procedure mimics the splitting of the valve leaflet with a surgical knife. How ever, there is no open-heart surgery in this The procedure is optimally performed with transesophageal echocardiography (TEE) guidance and under general anesthesia. An aortogram was performed to identify the arch vessels. The TMVR procedure was done with Cerebral Embolic Protection system to prevent cerebral stroke by deploying filters from the radial artery into the carotid (brain) artery. Any calcium particles or debris that may dislodge during the procedure are captured in these filters that effectively prevent cerebral stroke. Catheters was advanced from the femoral vein in the groin to the right side of the heart. Septal puncture was performed under TEE guidance. The wires woven through the catheter were advanced and positioned at the base of the mitral leaflet. The wires were electrified after confirming the position on TEE.
LAMPOON was performed successfully splitting the anterior mitral valve leaflet. The electrified wire acts as a knife, cutting the leaflet into two. The split was confirmed on TEE and a temporary pacemaker was placed from left common femoral vein. Balloon Septostomy was per formed. The new transcathe ter valve was advanced across the septum and positioned across the mitral annulus. The new valve was deployed. TEE showed normally function ing mitral valve. No increase in the LVOT gradients were seen. The cerebral protection system was removed after the implantation.
The patient was extubated (ventilator removed) immediately after the procedure and was transferred to ICU for observation. She could sleep comfortably in a supine (lying flat) position for the first time in 6 months.
Dr Ravinder Singh Rao said,” Lampoon procedure is a boon for patients who need a mitral valve replacement but are at high risk for an open-heart surgery. A strategic plan was made af ter carefully scrutinizing the challenges posed by obesity and LVOT obstruction. The safety and outcomes of such complex procedure depends on the experience of the team. The more the operator experi ence, the better are the safety outcomes of the procedure.” The above patient noticed the benefit of valve replacement very next day. She could sleep comfortably at night without any breathlessness and that she slept after many months. Next day she was able to walk with ease and noticed dramat ic improvement in her breath ing capacity. The valve starts functioning immediately in such patients and hence they notice immediate benefit.
Dr Rao and his team per formed this unique procedure of TMVR with antegrade LAMPOON without any complications which is rare and first of its kind in the country. Studies have shown that the outcomes of depends on the operator experience and expertise.