When it comes to cardio-vascular issues, it is important to weigh the pros and cons of available treatments, and choose the one that is right for you and your prognosis. However, we understand it can be intimidating and complex. Here we pose a discussion for an aortic valve stenosis, and the possible options for it. Here we weigh the merits and limitations of each therapy: TAVI and SAVR, to give you a broad discussion of each approach.
The Therapies
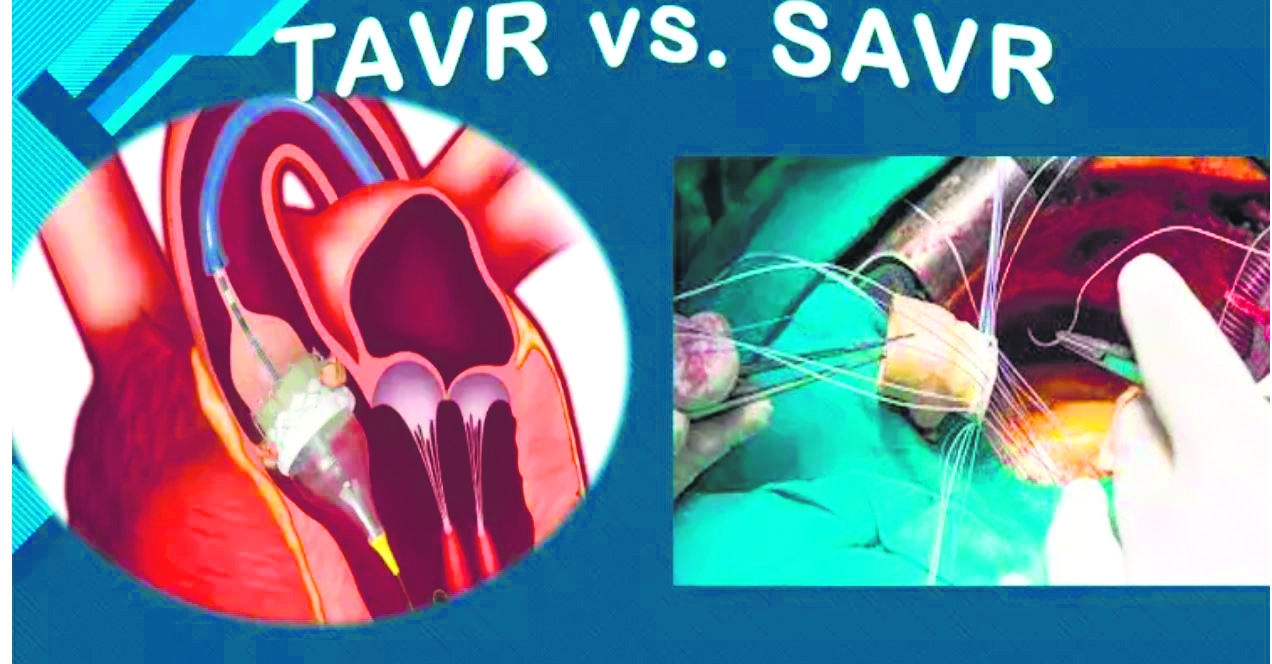
Transcatheter Aortic Valve Implantation (TAVI) and Surgical Aortic Valve Replacement (SAVR) represent two distinct approaches to treating aortic valve stenosis, a common cardiovascular condition characterized by the narrowing of the aortic valve opening. They are each chosen based on patient evaluation, depending on characteristics, risk profiles, and desired outcomes; and both have their merits.
TAVI also known as Transcatheter Aortic Valve Replacement (TAVR) is a minimally invasive procedure that involves inserting a new valve through a catheter, typically through the femoral artery in the groin area and involves no cut(incision) on the body and no ventilator while SAVR is an open-heart surgery that involves opening the chest, putting the patient on heart lung machine, ventilator support and removing the damaged valve and replacing it with a new one.
SAVR has long been the standard of care for patients with symptomatic severe aortic stenosis (AS). However, over the last decade, the emergence of TAVI has shifted the treatment paradigm from extreme-high-risk, to intermediate & low risk patients.
When TAVI started, it was the first-line therapy for severe aortic stenosis patients who cannot withstand an open-heart procedure. In fact, many of these patients had no hope of survival, until the introduction of TAVI.
TAVI is preferred in patients with co-morbidities, previous cardiac surgery, frailty, failed surgical bioprosthetic valve and restricted mobility. However, the research over the past decade has shown that TAVI is beneficial, safe and effective for patients who cannot easily undergo open heart surgery. For relatively younger patients, this fully percutaneous alternative to surgery is an attractive option with lower procedural risk, better quality of life and the possibility to return to work and a normal active life earlier relative to SAVR. As a result, the US FDA has approved TAVI as first line treatment for patients above the age of 65 years suffering from aortic stenosis. However, in India it is offered to even younger suitable patients also.
TAVI has become the treatment of choice for patients who have undergone a SAVR in the past with a tissue valve. The treatment is called “valve in valve” TAVI, wherein the new valve is inserted inside the failed SAVR valve, by going through the groin vessel.
It is important to note that the choice of procedure depends on several factors, including the patient’s age, overall health, and the severity of their aortic stenosis. It’s best to consult with a doctor to determine which procedure is right for you.





Merits:
The TAVI procedure has shown remarkable success in reducing mortality rates and improving the quality of life in high-risk to intermediate and low risk populations.
TAVI being a minimally invasive procedure ensures lower risk of infection and bleeding, shorter hospital stays, safer outcomes and a reduced recovery time as compared to traditional SAVR wherein the heart is stopped temporarily and put on a heart-bypass machine. TAVI is performed under local anaesthesia with conscious sedation, which avoids the risks associated with a general anaesthesia, particularly for people with other medical problems There is also no need for patients to be on an anticoagulant lifelong as compared to patients with mechanical valve from SAVR that are on lifelong anticoagulation therapy.
The TAVI technique also causes less fear and anxiety in patients, due to it being lower risk than the SAVR.
On the other hand, the SAVR is preferred in younger population who are at a lower surgical risk, those with small aortic annuli or have conditions such as aortic aneurysm or multivessel coronary artery disease. It is a durable option for younger patients who can undergo metallic valve implantation. SAVR allows for a comprehensive treatment of other associated heart problems, enabling simultaneous treatment of other cardiac conditions if present. The SAVR might also be used if the arteries are too small to accommodate the catheter that must be passed through till the heart.
With clinical studies there is data available from past 10 years which has proven that TAVI is superior to SAVR at preventing death, stroke, rehospitalization, major bleeding and renal failure events.
Limitations
The SAVR is a more invasive procedure and has a longer recovery period. Since there is a sternotomy involved, the patient requires more time to heal, and may spend a longer duration in the hospital. Moreover, the risks associated with open-heart surgery, like bleeding and infection, should be carefully considered when choosing between TAVI and SAVR.
While TAVI is less invasive, it is not without its limitations.
The outcome of TAVI procedure is directly related to the operator experience and expertise. More the TAVI experience and expertise, the safer are the TAVI outcomes. However, research is constantly being undertaken to improve long-term durability (at present limited to 10-15 years) of the TAVI valve and new technological advancements are being made every day for increased success and durability. The TAVI is a “Lifetime Management” protocol which needs to be followed for every patient with valvular disease.
Conclusion
There has to be the right balance between efficacy and invasiveness. Precision and customization are paramount in addressing the complexities of aortic valve stenosis. The choice between TAVI and SAVR is not a one-size-fits-all decision. Each therapy has its advantages and drawbacks, and the optimal choice depends on the unique characteristics of the patient. Ultimately, the goal is to enhance patient outcome, improve quality of life, and take care of individual needs in the ever-evolving cardiovascular landscape. Both the SAVR and TAVI procedures are a total clinical decision, and must only be taken by the doctor in question along with a discussion with the patient. TAVI has become a standard treatment for patients with failed SAVR tissues valve.
TAVI outcomes are dependent on the operator experience and expertise, with more experience associated with safer outcomes.
The author is a MBBS, MD, DM, FACC and Interventional Structural Cardiologist.